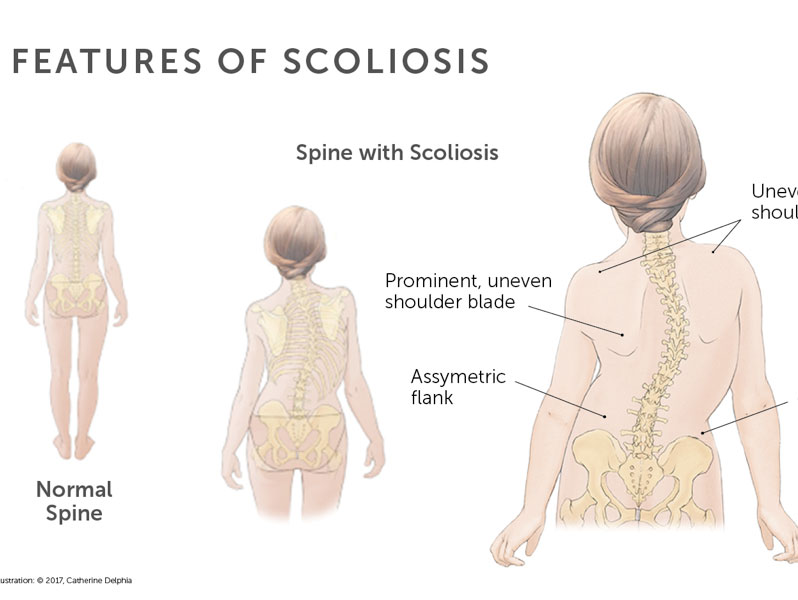
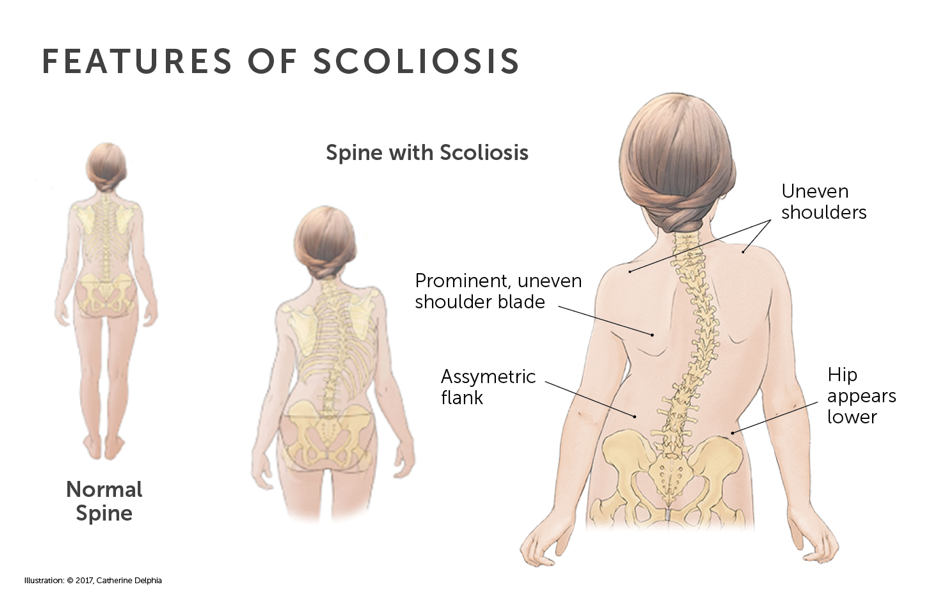
The group of diseases under the category of muscular dystrophy share some common characteristics, i.e. muscular weakness, atrophy (wasting) and development of contractures of the limbs. When the same weakness affects the muscles of the spine, often with some imbalance or asymmetrical involvement, scoliosis of the spine (curved spine) can result.
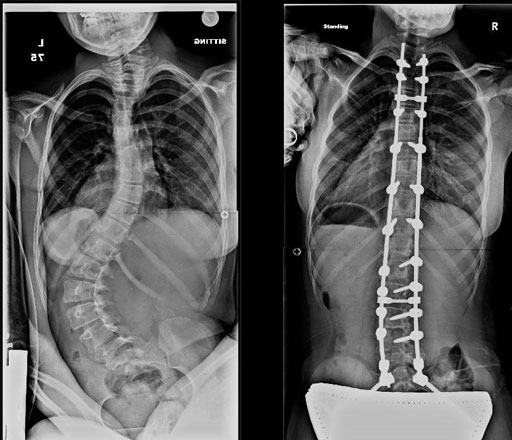
Scoliosis is one of the common complications of patients with muscular dystrophy who are only able to sit (non-walkers). For Duchenne Muscular Dystrophy (DMD), the scoliosis commonly develop and progress rapidly after they become wheelchair bound. For patients with Spinal Muscular Atrophy (SMA) where there are different forms with different severity, spinal deformities develop much earlier in non-walkers than in ambulant patients. In both DMD and SMA patients, the spinal curvatures are often thoracolumbar in location. Wheelchairs adapted with a firm seat and support is useful towards delaying the onset of scoliosis. On the other hand, marked spinal curvature may also make seating impossible. Forestalling or prevention of this complication is not always possible for some patients particularly when their ability to walk is lost. Although special body braces (spinal orthoses) have been tried, these were found to be ineffective in the management of neuromuscular scoliosis.
It is important to recognize the onset of scoliosis as it hinders adequate respiratory (breathing) functions. A curved spine results in restriction in the movement of the thoracic cage and thus, adversely affects respiratory capabilities. When wheelchair bound, patients should be encouraged to use incentive spirometry to maintain their respiratory efforts for as long as possible.